
I'm sure before too long we'll have a health forum and probably an education forum as well so I thought I'd kick them off with a rather controversial topic, Circumcision.
Now given the plethora of certain types of posters, (Macha are you reading this?) there could soon be acceptable reason to call for the reintroduction of circumcision.
Yes, it was news to me also, that circumcision was introduced as an aid in the prevention of masturbation ( yes, Macha, wanking!!)
The article was kindly stolen from a circo-site.
Read on and educate thyself!!
http://www.cirp.org/library/procedure/plastibell/
What were the original motivations behind routine infant circumcision in the West?
Routine circumcision as a preventative or cure for masturbation was proposed in Victorian times in America. Masturbation was thought to be the cause of a number of diseases. The procedure of routine circumcision became commonplace between 1870 and 1920, and it consequently spread to all the English-speaking countries (England, Canada, Australia and New Zealand). None of these countries now circumcise the majority of their male children, a distinction reserved today for the United States (in the UK, in fact, nonreligious circumcision has virtually ceased). Yet, there are still those who promote this social surgery, long after the masturbation hysteria of the past century has subsided.
"By about 1880 the individual... might wish[to]... tie, chain, or infibulate sexually active children... to adorn them with grotesque appliances, encase them in plaster, leather, or rubber, to frighten or even castrate them... masturbation insanity was now real enough--it was affecting the medical profession."
(B. Berkeley, quoted from _Circumcision: The Painful Dilemma_, by Rosemary Romberg, Bergin & Garvey Publisher, Inc, S. Hadley MA, USA, 1985, ISBN 089789-073-6)
Dr. E.J. Spratling, who promoted this surgery by telling his colleagues that "...circumcision is undoubtedly the physician's closest friend and ally..." prescribed in 1895 the method of circumcision as it is practiced in hospitals today.
"To obtain the best results one must cut away enough skin and mucous membrane to rather put it on the stretch when erections come later. There must be no play in the skin after the wound has thoroughly healed, but it must fit tightly over the penis, for should there be any play the patient will be found to readily resume his practice not begrudging the time and extra energy required to produce the orgasm... We may not be sure that we have done away with the possibility of masturbation, but we may feel confident that we have limited it to within the danger lines."
(E.J. Spratling, MD. Medical Record, Masturbation in the Adult, vol. 48, no. 13, September 28, 1895, pp. 442-443.)
Here is an example of what another sexaphobic American doctor had to say about masturbation in 1903:
"It (self abuse) lays the foundation for consumption, paralysis and heart disease. It weakens the memory, makes a boy careless, negligent and listless. It even makes many lose their minds; others, when grown, commit suicide.... Don't think it does no harm to your boy because he does not suffer now, for the effects of this vice come on so slowly that the victim is often very near death before you realize that he has done himself harm. It is worthy of note that many eminent physicians now advocate the custom of circumcision..."
(Mary R. Melendy, MD, The Ideal Woman - For Maidens, Wives and Mothers, 1903.)
(The above material is quoted from J. Bigelow, The Joy of Uncircumcising, Hourglass Book Publishing, Aptos, CA, USA. Thanks to Robin Verner.)
In America, foreskins were not rare at the time circumcision was introduced into widespread practice. Paradoxically, then, the understanding of the intact male organ at that time was somewhat greater than it is today. (In particular, it never would have been possible to promote circumcision on the basis that it was "necessary for hygienic reasons"---this came later, when doctors themselves were mostly circumcised men.)
Further, in proposing circumcision as a preventative against self-abuse, physicians of the day understood very well that male masturbation involves stimulation of the foreskin. However they were incorrect in assuming that, by reducing the pleasure, masturbation itself could be reduced or eliminated.
Porn Flakes:
Interestingly, Messrs. John Harvey Kellogg and Sylvester Graham (advocates of fibre, of both the moral and dietary varieties) were involved in this movement. Here's what Dr. Kellogg recommended:
A remedy for masturbation which is almost always successful in small boys is circumcision. The operation should be performed by a surgeon without administering an anesthetic, as the brief pain attending the operation will have a salutary effect upon the mind, especially if it be connected with the idea of punishment. In females, the author has found the application of pure carbolic acid to the clitoris an excellent means of allaying the abnormal excitement.
* What a sick bunch of cunts pouring acid on young girls genitals* PC
(John Harvey Kellogg, M.D., "Treatment for Self-Abuse and its Effects," Plain Fact for Old and Young. Burlington, Iowa: F. Segner & Co. (1888). P. 295) ...Isn't that enough to put you off Corn Flakes for the rest of your life? Visit this link for an essay by Carrie McLaren about Kellogg and Graham.
Circumcision in America, England and the other countries received a strong boost during each of the World Wars, because it was claimed that the procedure was necessary for soldiers for "hygienic reasons". Some soldiers who refused to be circumcised, were disciplined and/or received dishonourable discharges.
In 1949, the important work of Gairdner appeared in Britain, which led to the virtual cessation of medically-motivated circumcision in that country. Australia and New Zealand now also have very low rates (5% or less).
The largest problem remains in the United States, where the procedure has become culturally entrenched. The American public largely still believes circumcision to be a useful procedure, even though the rest of the world does perfectly well without it. It is worth noting that in 1996 the Canadian Paediatric Society issued a statement depreciating the value of circumcision in rather strong terms. Most Canadian provinces have dropped insurance coverage for circumcision, and the rest are expected to follow in the next year or so.
Circumcision never became an issue in continental Europe and in most of Asia, where the vast majority of men are intact. Religious circumcision is popular in some African, Muslim and Middle Eastern countries.
How is this genital reduction surgery perpetuated in the West today?
From its original roots in anti-masturbation hysteria, circumcision continues in English-speaking western countries (the United States, Canada, Australia and New Zealand) because of mistaken beliefs and unfounded fears about hygiene, disease, appearance and sexuality, and denial of the pain of infant circumcision. Please see the article Circumcision: A Medical or a Human Rights Issue? by Marilyn Fayre Milos, RN, and Donna Macris, CNM, MSN, in the Journal of Nurse-Midwifery, Vol.37,No.2 (Suppl.), March/April 1992.
For an excellent historical article detailing how circumcision became entrenched as a medical practice, see "From ritual to science: the medical transformation of circumcision in America", by David L. Gollaher, Journal of Social History, Fall 1994, vol. 28 no. 1, pp. 5-36
Anatomy of the Penis, Mechanics of Intercourse
This page presents information that most parents are not aware of at the time they make the circumcision decision. Doctors usually do not provide this information.
If you are under 18, we recommend that you share and discuss this information with your parents.
For a further look at this anatomy, including photographs, visit Circumstitions (Hugh Young). Hugh's site also includes an excellent animation to illustrate retraction.
Fig. 1. Intact adult penis
This illustration represents an average normal adult human penis. The head of the penis (glans) has a covering, called the foreskin (prepuce). This covering folds in on itself, forming a double layer. The foreskin is not a `flap' of skin on the end of the penis, and it is not `useless' or `redundant' skin.
There is some natural variation in the length of the foreskin, which often covers a bit more or less of the glans than illustrated.
In an average circumcised adult man, the area of skin that is missing because of penile reduction surgery would, when erect and unfolded, measure approximately three by five inches, or a little smaller than a postcard. That is about half the total skin of the penis.
Structures of the penis
The outer foreskin layer is a continuation of the skin of the shaft of the penis.
The inner foreskin layer is not just "skin," but mucocutaneous tissue of a unique type found nowhere else on the body.
The ridged band is the interface (join) between the outer and inner foreskin layers. When the penis is not erect, it tightens to narrow the foreskin opening. During erection, the ridged band forms ridges that go all the way around, about halfway down the shaft.
The reddish or purplish glans or glans penis (head of the penis) is smooth, shiny, moist and extremely sensitive.
The frenulum, or frenum, is a connecting membrane on the underside of the penis, similar to that beneath the tongue. Fig. 2. Intact penis (hidden structures shown).
The foreskin has twelve known functions.
They are:
1. to cover and bond with the synechia so as to permit the development of the mucosal surface of the glans and inner foreskin.
2. to protect the infant's glans from feces and ammonia in diapers.
3. to protect the glans penis from friction and abrasion thoughout life.
4. to keep the glans moisturized and soft with emollient oils.
5. to lubricate the glans.
6. to coat the glans with a waxy protective substance.
7. to provide sufficient skin to cover an erection by unfolding.
8. to provide an aid to masturbation and foreplay.
9. to serve as an aid to penetration.
10. to reduce friction and chafing during intercourse.
11. to serve as erogenous tissue because of its rich supply of erogenous receptors.
12. to contact and stimulate the G-spot of the female partner.
The above list was compiled from various sources by George Hill.
Click here for more information about the skin system of the penis.
Fig. 3: Erection process: Intact penis
When fully retracted, the foreskin is designed to cover essentially the entire penile shaft, yet is loose enough to "glide". The ridged bands are situated about halfway down the shaft, when the foreskin is retracted fully.
Note: In some cases, a man may have difficulty retracting the foreskin. This is not an indication for circumcision, because there are good alternative treatments available that preserve the structure and function of the foreskin. Scientific references for information on this topic can be found in CIRP's Circumcision Reference Library.
See also the excellent animation at Circumstitions.com (offsite link).
Penile stimulation
The most important components of the physical erogenous stimulation of the penis during foreplay and intercourse are the sensations from the foreskin, frenulum/frenar band, and glans. These structures each have their own feeling, and each contributes in its own way to the man's total experience of lovemaking. It must be emphasized that emotional excitement is an extremely important component of sexual enjoyment, and intensifies the man's perception of any physical sensations from his penis.
The foreskin has an inner and outer layer. The outer foreskin layer contains nerve endings which respond to gentle touching during the early stages of sexual arousal. This helps to trigger an erection. The nerves of the inner and outer foreskin contribute to the experience of penile stimulation, up to and including orgasm. These receptors are stimulated by stretching, or when the foreskin rolls over the surface of the glans during intercourse or masturbation. (see `the gliding mechanism,' below).
The foreskin contains sensory receptors called Meissner corpuscles. We believe that these nerves, similar to nerve endings in the fingertips, are there to provide pleasure, as well as fine sensory perception. This seems to help a man to enjoy sex longer without ejaculating prematurely, because he can more easily tell when he is approaching the threshold of orgasm.
Stimulation of the frenulum and ridged band results in intense pleasurable feelings during arousal. The ridged band consists of a number of "ridges", described by Dr. John Taylor in his recent article. Sensations from these structures during intercourse or masturbation are thought to be the primary trigger of orgasm in the intact male. Dr. George Denniston writes:
The ridged bands, which are like horseshoes only in that they curve forward underneath toward the point where the frenulum attaches, can be found in several pictures in John's paper. There are some 20 concentric ridged bands which rub over the corona. Each ridge has Meissner's corpuscles, which respond to pressure, and they produce the sexual pleasure which no individual has a right to take away from another individual.
We believe that stimulation of the glans is most significant in the later stages of sexual intercourse, when penetration is deepest and emotions are running at their highest. Sensations from the glans contribute to the quality of the sensual experience. They are also apparently capable of triggering orgasm on their own, as would be the case in a circumcised man.
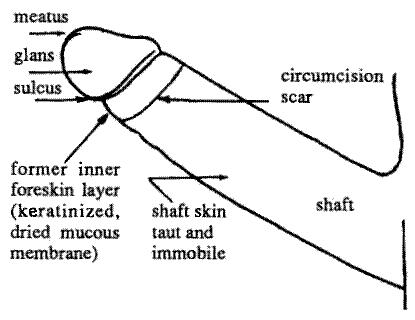
Fig. 4. Circumcised adult penis
Fig. 5. The circumcised penis: Erect state
Following circumcision, the foreskin of the penis has been cut away. The surface of the glans has developed a thick, dry layer of keratin (toughened skin), which makes it less sensitive to unwanted stimulation, but also less sensitive to the more subtle qualities of lovemaking.
All circumcised men have an annular scar on the shaft of the penis. The location of the scar varies, from near the head to far down the shaft. For some men, so much skin has been removed that erection becomes difficult and even painful. This was one of the most common complaints reported by circumcised men in a recent poll.[11]
The gliding mechanism
During intercourse the loose skin of the intact penis slides up and down the shaft of the penis, stimulating the glans and the sensitive erogenous receptors of the foreskin itself. On the outstroke the glans is partially or completely engulfed by the foreskin. This is known as the `gliding mechanism.'
The gliding mechanism is Nature's intended mechanism of intercourse. As such, it contributes greatly to sexual pleasure. Also, since more of the loose skin of the penis remains inside the vagina, the woman's natural lubrication is not drawn out to evaporate to a great extent, which makes sex easier without using artificial lubricants.
The prepuce is a highly innervated and vascularized genital structure. It is entirely lined with the peripenic muscle sheet. Specialized ecoptic sebaceous glans on the inner preputial surface produce natural emollients and lubricants necessary for normal sexual function. The primary orgasmic triggers are found in the preputial orifice and frenulum. When unfolded, the prepuce is large enough to cover the length and circumference of the erect penis and acts as a natural sheath through which the shaft glides during coitus. Only the presence and functions of the prepuce allow for physiologically normal coitus to occur as designed by nature.
(Fleiss, Paul M; Frederick Hodges. "Nontherapeutic Circumcision Should not be Performed," American Medical News, vol. 38, no. 26 (July 17, 1995): p. 16.) Fig. 6. The gliding mechanism
Effects of penile reduction surgery (circumcision) on sexual intercourse
Although still pleasurable for the man, intercourse without the participation of the prepuce lacks the gliding mechanism. The only source of stimulation is the glans rubbing against the wall of the vagina. The sensations from the specialised receptors of the frenar band, frenulum and inner foreskin layer are missing.
"With intravaginal containment of the normal penis, the male's mobile sheath is placed within the woman's vaginal sheath. It is impossible to imagine a better mechanical arrangement for non-abrasive stimulation of the male and female genitalia than this slick 'sheath within a sheath.' Circumcision destroys this one sheath within a sheath . . . I would hazard a guess, that dyspareunia [painful intercourse] is more common in the women whose husband is circumcised . . . one would be foolish to discount the circumcised male's immobile penile skin sheath as an ancillary item contributing to vaginal, abrasive discomfort . . . The male with a penis already moderately obtunded by circumcision may be less apt to use a condom, which he feels may further decrease his genital sensitivity . . . because most American males lack a facile prepuce, the period of foreplay and dalliance may be abbreviated in the rush to the intra-vaginal method of penile stimulation. Both these factors conceivably could be of significance in increasing the rate of venereal disease, including AIDS . . . "
(Say No to Circumcision! 40 Compelling Reasons Why You Should Respect His Birthright and Leave Your Son Whole (2nd edition), by Thomas A. Ritter, MD, Hourglass Book Publishing 1996)
If the surgery was performed on an infant, by adulthood a relatively thick keratin layer will have formed on the normally skinless mucosal surface of the glans, which further reduces the stimulation. If the circumcision was performed as an adult, the keratin layer will form, and the sensitivity of the glans will gradually be reduced over time.

Results 1 to 13 of 13
Thread: The Health and Education Thread
-
26-06-2005, 02:10 PM #1Aspiring Guru








- Join Date
- Jun 2005
- Last Online
- 27-07-2006 @ 09:21 PM
- Location
- pratunam
- Posts
- 4,456
The Health and Education Thread
-
26-06-2005, 02:30 PM #2
R.I.P.

- Join Date
- Jun 2005
- Last Online
- @
- Location
- Pattaya Jomtien
- Posts
- 58,763
hmmmmm, i really dont know wot to say, i assume that have wanted to post that for quite a while pool cleaner, well at least you have got it out of your system now...

-
26-06-2005, 02:51 PM #3Thailand Expat

- Join Date
- Jun 2005
- Last Online
- 08-09-2014 @ 10:43 AM
- Location
- Simian Islands
- Posts
- 34,827
So, it's OK to have dick-cheese?6. to coat the glans with a waxy protective substance. ops:
ops:
-
26-06-2005, 03:50 PM #4Aspiring Guru
- Join Date
- Jun 2005
- Last Online
- 27-07-2006 @ 09:21 PM
- Location
- pratunam
- Posts
- 4,456
Well actually no! Originally Posted by dirtydog
Originally Posted by dirtydog
This topic was brought up last night during beers and when I googeld today this was the first site I went to and I was impressed!!
But I do feel more comfortable raising delicate topics in our new environment where I feel they will find a far more mature reception than in the past.
For this we have you to thank dd.
If the general banter in girlie bars and short time hotels shows a marked improvement it will be down to your forsight in creating this vital and dynamic forum.
:idea:
-
26-06-2005, 04:19 PM #5Thailand Expat
- Join Date
- Jun 2005
- Last Online
- 20-09-2006 @ 09:55 PM
- Posts
- 2,975
Originally Posted by Dennis the Dictionary
-
26-06-2005, 04:23 PM #6Aspiring Guru
- Join Date
- Jun 2005
- Last Online
- 27-07-2006 @ 09:21 PM
- Location
- pratunam
- Posts
- 4,456
Originally Posted by Captain Sensible
Is there a TeakDoor diplomatic vacancy?
I'm rather good at blowing smoke up people's bums, apparently!
-
26-06-2005, 05:12 PM #7Thailand Expat
- Join Date
- Jun 2005
- Last Online
- 20-09-2006 @ 09:55 PM
- Posts
- 2,975
How are you at tossing a salad Poolie? :?
I could see you as a cultural attache actually. :P
-
26-06-2005, 08:04 PM #8Aspiring Guru
- Join Date
- Jun 2005
- Last Online
- 27-07-2006 @ 09:21 PM
- Location
- pratunam
- Posts
- 4,456
Oh dear! Originally Posted by Captain Sensible
Wasn't Bazza McKenzie one of them?
I shall do my best to bring exciting, relevant and interesting topics to the populace of TeakDoor!
No, it's not socks and feet for me. I will endeavour to create threads with substance.
How about "Piccy's of your scabbiest soi dogs and cats"
I like piccy threads. Especially Thai topics so we can bring our world to the less fortunate living in the UK or the US.
Any ideas let me know!!
-
26-06-2005, 08:11 PM #9
R.I.P.
- Join Date
- Jun 2005
- Last Online
- @
- Location
- Pattaya Jomtien
- Posts
- 58,763
i have been meaning to take pics of dogs that have been killed on the road, you know the sort of stuff, intestines spread across the highway sort of thing and fun stuff like that, i just never seem to have the time once the owners have seen that i have run over their mangy dog
-
27-06-2005, 07:07 AM #10Newbie

- Join Date
- Jun 2005
- Last Online
- 15-12-2008 @ 09:11 PM
- Posts
- 46
Thanks a lot Pooly, There are a few facts about dicks I didn't know.

-
27-06-2005, 07:11 AM #11Thailand Expat
- Join Date
- Jun 2005
- Last Online
- 20-09-2006 @ 09:55 PM
- Posts
- 2,975
Good morning Butch. :P I see you got the door open mate. Welcome.
-
27-06-2005, 08:46 AM #12Aspiring Guru
- Join Date
- Jun 2005
- Last Online
- 27-07-2006 @ 09:21 PM
- Location
- pratunam
- Posts
- 4,456
Originally Posted by GC
*message to dirtydog: are you reading this?*
Thanks GC.
My aim is to inform and educate 8)
-
30-06-2005, 10:17 PM #13Aspiring Guru
- Join Date
- Jun 2005
- Last Online
- 27-07-2006 @ 09:21 PM
- Location
- pratunam
- Posts
- 4,456
A couple of members have pmed me this week asking..
"Pooly, what do you know about vaginal prolapses?"
My initial reply was "Well you certainly wouldn't want one!"
read on but be warned, it's not for the faint hearted!
Don't open these in a sensitive environment, you'll never be able to explain
http://www.ogrish.com/archives/2004/...om-Scan6sm.jpg
http://www.ogrish.com/archives/2004/...om-Scan7sm.jpg
http://www.ogrish.com/archives/2004/...prola_pso6.jpg
http://www.ogrish.com/archives/2004/...prola_pso7.jpg
VAGINAL PROLAPSE - a patient's guide
Dr Mark Insull - Gynaecologist
What is it?
Genital tract prolapse can be defined as weakness of the supporting structures of the uterus, pelvic floor and vagina. This condition affects up to 30 to 40 percent of all women and is certainly one of the more common reasons why women over the age of 40 present for gynaecological assessment and care.
What does genital tract prolapse involve?
Weakness in the front (cystocele) and/or back (rectocele) walls of the vagina
Weakness of the supports to the uterus (prolapse of the uterus)
Weakness in the upper part of the vagina which can cause a hernia (enterocele)
What causes this condition?
Childbirth - prolonged labours and in particular, prolonged 2nd stage labour, and big babies.
Menopause - decreasing oestrogen levels have an impact on the collagen content of the pelvic floor tissues.
Hereditary genetic predisposition to this condition - many women have large babies with long labours, go through menopause and do not have a prolapse.
What symptoms do women present with?
Some women are asymptomatic - in other words they have no symptoms at all and the prolapse or weakness in the genital tract is noted on a routine examination.
More commonly a woman may present with a history of noticing a lump at the entrance to her vagina which may be, either her cervix (which is the bottom part of the uterus) or the front and back walls of the vagina which have prolapsed down through the entrance to the vagina.
There maybe a dragging sensation in the lower pelvis and/or backache.
Stress incontinence - which is leakage of urine when coughing, sneezing, laughing or during exercises.
The need to place a finger in the vagina when having a bowel motion to reduce the prolapse and thus make passing a bowel motion a little easier.
At what age does this problem become more common?
While many women do notice temporary symptoms of prolapse such as a lump to the entrance to the vagina and/or stress incontinence following delivery of a baby, these symptoms often significantly improve with the passage of time and/or physiotherapy.
The most common age group are those women who are experiencing menopause, usually over the age of 50, although all age groups may be affected.
How is the problem treated?
Taking a careful history of the symptoms will give a very good guide to what is going on.
Examination will confirm whether the prolapse is involving the vaginal walls and/or the uterus - in most cases it is unusual to find an isolated defect or weakness in one part of the pelvic floor, but rather a general weakness. It is important that all areas of genital tract prolapse are repaired.
Physiotherapy - pelvic floor exercises can be very useful in those women with mild degrees of prolapse and/or stress incontinence. Perseverance and professional help with these exercises is important.
In selected patients, particularly when older and not wishing to be sexually active, or who cannot have surgery because of heart disease or other medical problems, a vinyl ring pessary can be inserted onto the vagina which will hold the prolapse back. This has the disadvantage of making intercourse very difficult and at times causing ulceration to the vagina due to pressure from the ring on the vagina. However, it is an effective treatment for those groups described above and many patients will be satisfied with the help a ring pessary can give.
Surgery
If conservative measures fail to improve the situation, the options of surgery may be discussed with a gynaecologist. The following operations are available:
An anterior colporrhaphy or repair - tightens up the front walls of the vagina.
Prosterior repair or prosterior colporrhaphy - tightens up the back wall of the vagina.
Hysterectomy (removal of the uterus) is usually performed through the vagina if significant uterine prolapse is present.
If stress incontinence (leakage of urine with coughing or sneezing) is present, a laparoscopic incontinence procedure called a Laparoscopic Burch colposuspension is favoured.
Increasingly, laparoscopic surgery is used to tighten up the back wall of the vagina, to repair hernias involving the top of the vagina (enteroceles), and to support the top of the vagina after a hysterectomy if it becomes weakened.
How long will I be in hospital for?
Usually two to four days depending on the type and extent of surgery involved. The only significant restriction postoperatively would be the need to avoid heavy lifting for approximately six weeks.
What are the long term results like?
Results following prolapse surgery are usually very good, whether performed through the vagina or with the aid of the laparoscope, with excellent patient satisfaction.
The tissues in the area that are being operated on are not as strong as they used to be, otherwise the prolapse would not have occurred, therefore there is still a slight risk of occurrence of the prolapse in the future. The risk of recurrence of the prolapse can be reduced by making sure that all pelvic floor defects are treated at the time of the initial surgery and that appropriate surgery is performed based on the clinical findings.
Seeking help
Many women delay seeking help for this condition due to embarrassment; this should not be the case as effective and sympathetic treatment should be available through you gynaecologist or family doctor.







 Reply With Quote
Reply With QuoteThread Information
Users Browsing this Thread
There are currently 1 users browsing this thread. (0 members and 1 guests)
